Combination Antiemetic Regimens
A summary of possible antiemetic regimens, based on the emetic potential of the chemotherapy regimen:
Serotonin antagonist plus dexamethasone: Drug combinations involving a 5-HT3 antagonist and dexamethasone have demonstrated to be the most effective treatment regimens for managing acute chemotherapy-induced emesis. Combined use of these agents has shown to be more effective as compared to single use of either of these agents. When an NK1 antagonist (aprepitant) is added to this combination, it leads to increased activity against acute chemotherapy-induced emesis. However, a reduced dose of concomitantly administered dexamethasone may be necessitated due to the inhibition of the CYP3A4 metabolic pathway by aprepitant.
Treatment Options for Emesis
Acute Emesis
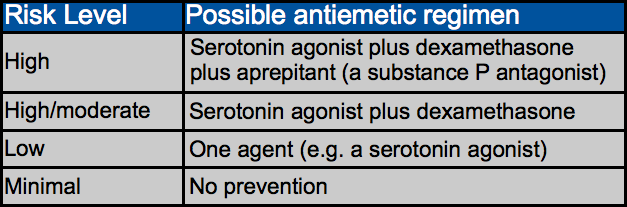
The table below summarizes a treatment strategy for the prevention of acute chemotherapy-induced emesis. Experts recommend that all patients be given education and reassurance, and also antiemetics tailored specifically to suit the chemotherapy regimen. Antiemetic combinations are recommended in case of regimens that often cause emesis (>30%), whereas a single agent is considered sufficient in case of low-risk regimens (incidence of 10-30%). Preventive treatment is not usually given in case of minimal risk chemotherapy.
Delayed Emesis
This refers to nausea and vomiting that begins or persists ≥ 24 hours after chemotherapy is administered. The pathophysiology of this condition may not be clear, but it has been noticed that it occurs mostly after high-dose cisplatin, doxorubicin, cyclophosphamide, or carboplatin. Both cisplatin and carboplatin are often used in treatment of mesothelioma.
A study found that approximately 89% of patients who received high-dose cisplatin experienced some delayed emesis between 24-120 hours, with a peak occurrence recorded between 48-72 hours. In case of cyclophosphamide or anthracyclines, the delayed emesis rate without preventive antiemetics is around 30%.
Delayed emesis can begin earlier. In cases wherein there is failure of combination antiemetic regimens used to control acute emesis, the initial emetic response often occurs between 17-23 hours after chemotherapy is administered
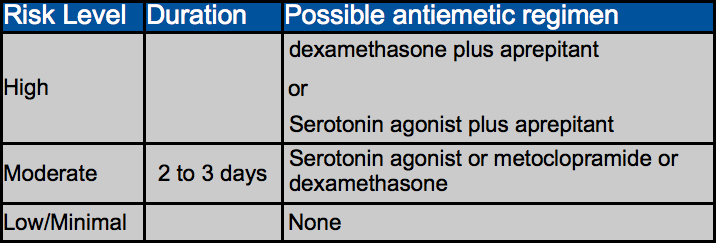
Treatment. It has been shown that the combination of oral dexamethasone and metoclopramide is more effective than dexamethasone alone or a placebo. Also found to be effective is the combination of dexamethasone and aprepitant. The effect of palonosetron can also last for several days.
Anticipatory Emesis
Anticipatory emesis is nausea or vomiting that begins prior to the administration of chemotherapy among patients who have had experienced poor emetic control during earlier courses of chemotherapy. This is a conditioned response, and treatment-related associations including just being in the hospital can lead to emesis. Poor emetic control combined with strong emetic stimuli can increase the chances of the potential occurrence of anticipatory emesis.
Treatment. It has been demonstrated that behavioral therapy involving systematic desensitization is useful in managing anticipatory emesis. Benzodiazepines have also been found to be effective. However, prevention is the most appropriate approach. This necessitates that the most potent and appropriate antiemetic regimens be used with the primary course of emesis-producing chemotherapy.
Mesothelioma Aid Support Topics
Financial Planning for Cancer Patients
Free Information Packet on Mesothelioma
If you would like to receive a FREE information packet on mesothelioma**, or if you have a comment or question, please complete the following:
**(Packet includes information on treatment, clinical trials, cancer links, how to access legal and financial resources, and frequently asked legal questions with answers provided by Cooper, Hart, Leggiero & Whitehead, PLLC). By filling out the above form you consent to being contacted by Cooper, Hart, Leggiero & Whitehead regarding potentially retaining legal services.